Vi använder cookies för att ge dig bästa möjliga upplevelse. Välj vilka cookies du tillåter.
Läs mer i vår integritetspolicy
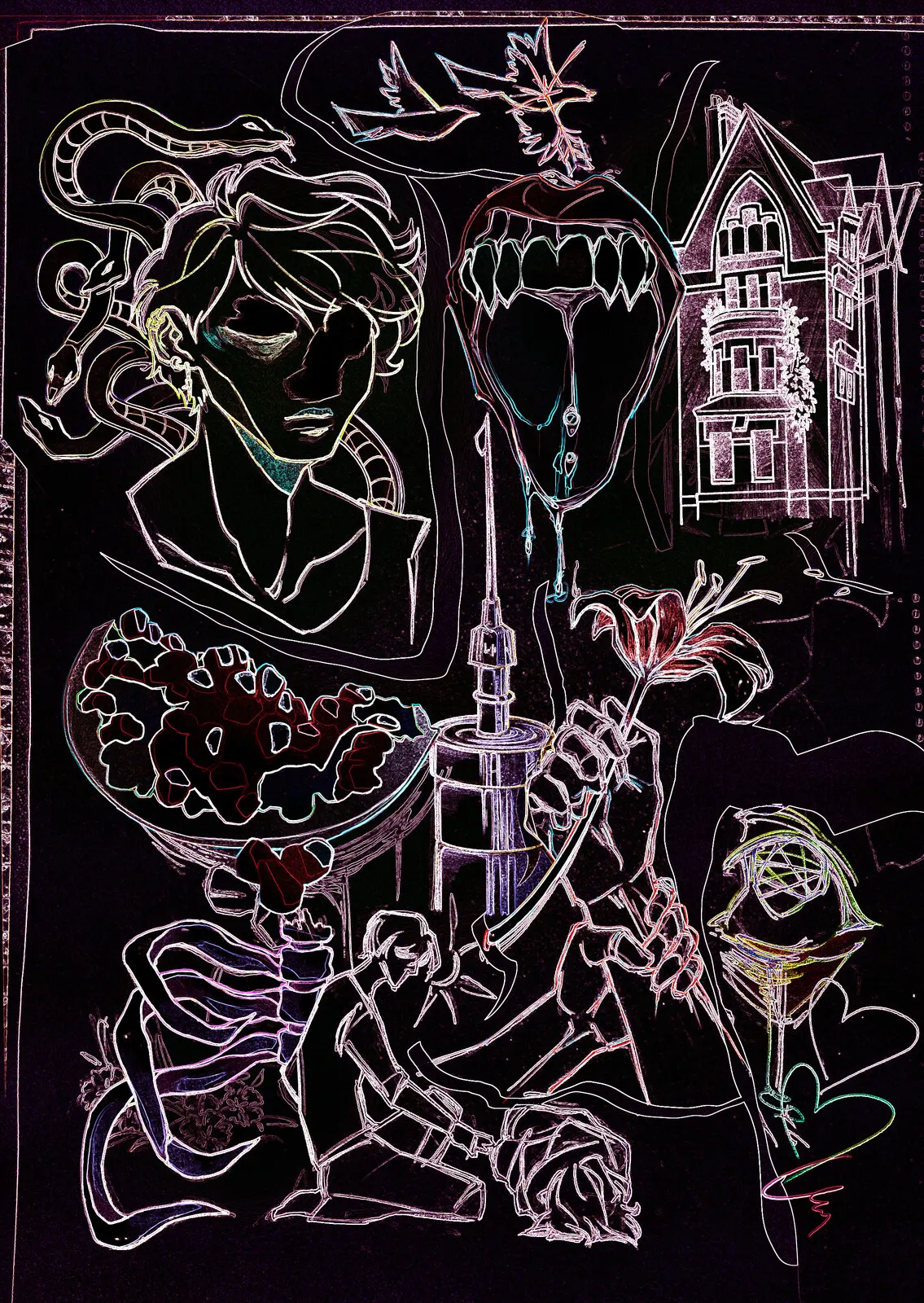
Maria Malm
Lily, love and family, 2025
Blandteknik
During the 1700-1800s, female hysteria was one of the most common mental disorders to be diagnosed. It was a condition that could readily be applied to any display of behaviours deemed “difficult”.
As far back as the 16th century it has been a completely justified approach to simply lock away those deemed noncompliant with societal norms. Groups like these included the mentally ill, poor, homeless, elderly and of course women threatening the patriarchy simply by defying the contemporary view of femininity and what it meant to be a woman. Since male medical professionals deemed the female nature to be one of contempt, submission and codependence, any display of behaviours that deviated from these were enough to brand a woman as insane and have her admitted to a mental institution. Further, most men in the field assumed that womanhood was at some level inseparable from mental instability as they held the belief that female insanity and hysteria could be directly linked to the reproductive system, and especially the uterus. Possession of normal female body parts therefore posed an innate risk for mental illness. This made it perfectly reasonable to institutionalize women because of incredibly common, sometimes unavoidable, occurrences such as lack of a menstrual cycle, a misscarriage and early onset of menopause.
Typically the practice of institutionalizing women was performed by their husbands as a form of domestic abuse. Early on in psychiatry there were no guidelines or regulations to assess a woman’s mental state which left the final assessment to be made by her husband or a male relative. This power was often abused and functioned as a device for men to threaten or deal with their “difficult” wives in domestic disputes. Women were the possession of their husbands and if they ceased to fulfill their proper function they were viewed as a broken tool or instrument that simply could be fixed through institutionalization, or be replaced. It never seemed to occur that these problems possibly could be caused due to poor living conditions such as isolation from anyone but one’s husband and children, mental and physical abuse and an unequal distribution of labour and expectations in the home. Other valid reasons to declare a woman insane included insanity induced by childbirth, an inability to fulfill her motherly duties, any expression of sexuality or enjoyment of sex or an inability or refusal to please her husband.
Of course unmarried women were in no better position as their defiance of the institution of marriage itself was seen as a major offence and moral failure. Single women would more often suffer the negative backlashes of failing to meet the societal expectations of women in the form of psychological ostracization. Lesbians automatically deviated from the established definition of a woman, namely a creature dependent on male affiliation to remain sane. Without continuous male interaction doctors claimed that women could start to suffer from anemia, irritability and tiredness. To live and move freely outside alone or with another woman was strictly taboo behaviour and cause for treatment.
As mentioned, male professionals in the medical field have throughout history persistently claimed the female physique to be the main cause for enhanced susceptibility to mental illness in female patients. This argument has been used to deny women independence, places in academia and any field of work outside of the household, proper medical care and the ability to make choices in regards to their own bodies. Whether or not properly educated physicians and doctors actually believed that women were innately less mentally stable simply due to the nature of the female body is unclear. Surely some did. Regardless, many physicians and gynecologists at the time were incentivized to adhere to this belief as many of these men were the very same as the ones who owned the asylums and institutions profiting from the high influx of patients. Therefore, many women, sane or not, would be recommended institutionalization, not with the intent of treating any real or made up mental illnesses, but rather as a carefully orchestrated strategy by the patriarchal psychiatric community to remain in control. It was simply more profitable for these men not to address and treat any real concerns and rather play into the imagined ones. By linking femininity to innate inanity the system would simultaneously reinforce the physicians’ authority on the topic while discarding any opposition by completely reasonable women as hysteria.
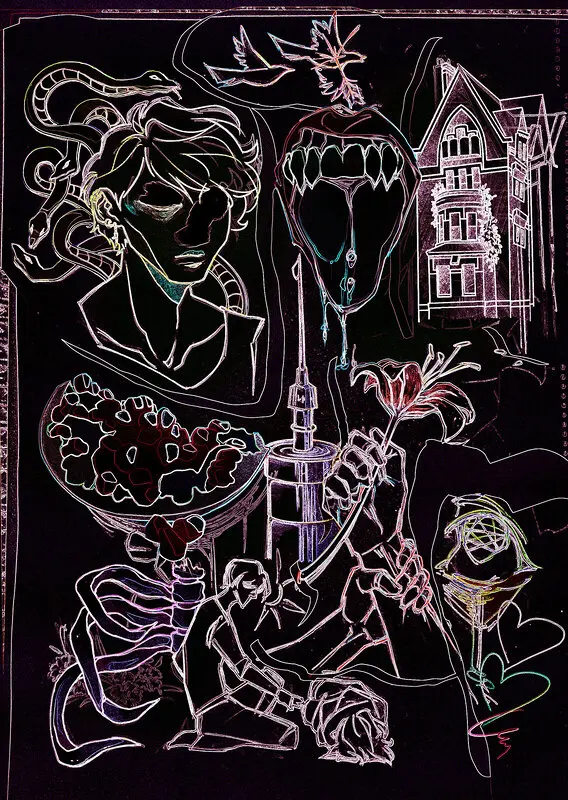
Maria Malm
Lily, love and family, 2025
Blandteknik
During the 1700-1800s, female hysteria was one of the most common mental disorders to be diagnosed. It was a condition that could readily be applied to any display of behaviours deemed “difficult”.
As far back as the 16th century it has been a completely justified approach to simply lock away those deemed noncompliant with societal norms. Groups like these included the mentally ill, poor, homeless, elderly and of course women threatening the patriarchy simply by defying the contemporary view of femininity and what it meant to be a woman. Since male medical professionals deemed the female nature to be one of contempt, submission and codependence, any display of behaviours that deviated from these were enough to brand a woman as insane and have her admitted to a mental institution. Further, most men in the field assumed that womanhood was at some level inseparable from mental instability as they held the belief that female insanity and hysteria could be directly linked to the reproductive system, and especially the uterus. Possession of normal female body parts therefore posed an innate risk for mental illness. This made it perfectly reasonable to institutionalize women because of incredibly common, sometimes unavoidable, occurrences such as lack of a menstrual cycle, a misscarriage and early onset of menopause.
Typically the practice of institutionalizing women was performed by their husbands as a form of domestic abuse. Early on in psychiatry there were no guidelines or regulations to assess a woman’s mental state which left the final assessment to be made by her husband or a male relative. This power was often abused and functioned as a device for men to threaten or deal with their “difficult” wives in domestic disputes. Women were the possession of their husbands and if they ceased to fulfill their proper function they were viewed as a broken tool or instrument that simply could be fixed through institutionalization, or be replaced. It never seemed to occur that these problems possibly could be caused due to poor living conditions such as isolation from anyone but one’s husband and children, mental and physical abuse and an unequal distribution of labour and expectations in the home. Other valid reasons to declare a woman insane included insanity induced by childbirth, an inability to fulfill her motherly duties, any expression of sexuality or enjoyment of sex or an inability or refusal to please her husband.
Of course unmarried women were in no better position as their defiance of the institution of marriage itself was seen as a major offence and moral failure. Single women would more often suffer the negative backlashes of failing to meet the societal expectations of women in the form of psychological ostracization. Lesbians automatically deviated from the established definition of a woman, namely a creature dependent on male affiliation to remain sane. Without continuous male interaction doctors claimed that women could start to suffer from anemia, irritability and tiredness. To live and move freely outside alone or with another woman was strictly taboo behaviour and cause for treatment.
As mentioned, male professionals in the medical field have throughout history persistently claimed the female physique to be the main cause for enhanced susceptibility to mental illness in female patients. This argument has been used to deny women independence, places in academia and any field of work outside of the household, proper medical care and the ability to make choices in regards to their own bodies. Whether or not properly educated physicians and doctors actually believed that women were innately less mentally stable simply due to the nature of the female body is unclear. Surely some did. Regardless, many physicians and gynecologists at the time were incentivized to adhere to this belief as many of these men were the very same as the ones who owned the asylums and institutions profiting from the high influx of patients. Therefore, many women, sane or not, would be recommended institutionalization, not with the intent of treating any real or made up mental illnesses, but rather as a carefully orchestrated strategy by the patriarchal psychiatric community to remain in control. It was simply more profitable for these men not to address and treat any real concerns and rather play into the imagined ones. By linking femininity to innate inanity the system would simultaneously reinforce the physicians’ authority on the topic while discarding any opposition by completely reasonable women as hysteria.

Maria Malm
Linköping
För att se vad mer jag håller på med besök: mariamalm.webnode.se/